
A 34-year-old Caucasian female with a PMH of HTN and HLD presenting to the emergency department with chest pain x 1 day
HPI:
- Patient was sitting at home, watching tv in bed when pain started at approx. 1700 yesterday
- Pain is right-sided, located under the breast, described as stabbing, radiates to her upper back, worse when she takes a deep breath
- She hasn’t taken any medications for the pain. Changing positions doesn’t make pain better
- Endorses shortness of breath that occurs when ambulating around her apartment, started at the same time yesterday
- Has never experienced similar symptoms in the past
- Reports she had surgery to repair Achilles tendon rupture two weeks ago
- Denies fever, chills, headache, diaphoresis, cough, abdominal pain, nausea, vomiting, diarrhea.
- Denies recent long car rides/flights
- Denies history of blood clots
PMH: HTN, HLD
Meds: OCP, Lisinopril 5 mg PO daily
Allergies: NKDA
Social: Lives in apartment with her husband and 2 kids. Would like to have another child. Glass of wine with dinner every night, quit smoking 4 years ago when first kid was born. Previous 7year pack history. Denies illicit drug use.
Family Hx: Dad died of “some heart thing” 20 years ago. Mom alive, 68 years old, has HTN
Vaccines: Received annual flu vaccine in October 2021. Received 3 x Moderna COVID vaccines (booster in January 2022).
PE:
- Vitals: BP 125/79, P102, RR18, T99.1F, O2 95% on RA, BMI 31
- General: A&Ox3. NAD, appears comfortable
- Respiratory: Nontender to palpation, CTAB, symmetric chest expansion
- Cardiac: Tachycardic, regular rhythm, no murmurs, 2+ radial pulses bilaterally, normal capillary refill
- Abdomen: +BS, non-distended, non-tender
- Extremities: No calf tenderness, 2+ DP pulses bilaterally, 1+ pitting edema left leg
- Skin: Warm and dry, no erythema
Differential Diagnosis and Justification:
- Pulmonary embolism
- Wells’ Score 9 (high risk)
- PERC score 4 (tachy, unilateral leg swelling, recent surgery, OCP use)
- Myocardial Infarction
- Female, exertional chest pain, history of HTN/HLD, obese BMI, tachycardic, HEART score 3 (low)
- Aortic dissection
- Stabbing chest pain radiating to the back, ADD-RS score 1 (get D-dimer)
Labs/Tests to Order:
- EKG
- CBC, BMP, PT/PTT, urine hCG, troponin, D-dimer
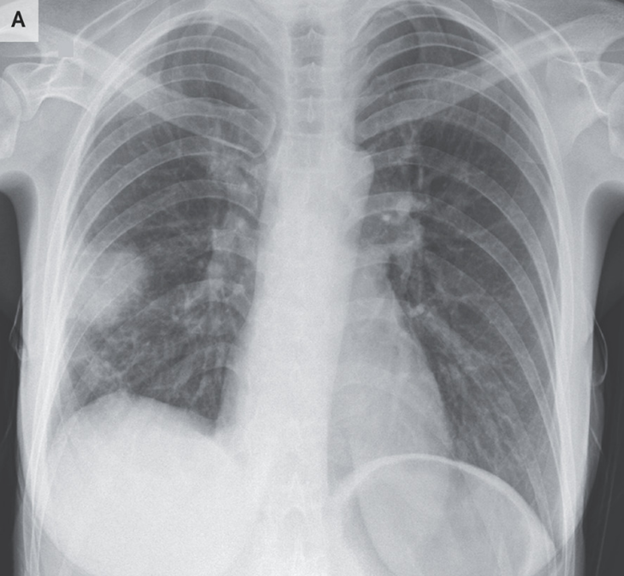
- CXR
- US of lower extremity
- CT-chest if D-dimer positive
Lab/Test Results:
- EKG: Sinus tachycardia
| WBC | 12.5 |
| Hgb | 11.4 |
| Hct | 35.7 |
| Plt | 346 |
| Na | 142 |
| K | 4.1 |
| Cl | 104 |
| CO2 | 25 |
| BUN | 10 |
| Cr | 0.7 |
| Glu | 84 |
| PT | 13.5 sec (normal) |
| PTT | 30 sec (normal) |
| INR | 1.1 (normal) |
- Urine hCG: Negative
- Troponin: Normal (non-elevated)
- D-dimer: Positive
- CXR: Shown below
- US: Unavailable until the morning
- CTA with contrast: Multiple small emboli in distal right pulmonary vasculature
Treatment:
- Admission for anticoagulation
- Xarelto (Rivaroxaban) 15mg PO BID for 21 days
- Followed by 20mg PO QD with food for 3 months
- (No contraindications and does not require bridging therapy)
- Acetaminophen 325mg, 2 tablets, PO PRN for chest pain
- Xarelto (Rivaroxaban) 15mg PO BID for 21 days
Patient Education:
- Follow-up care is a key part of your treatment and safety.
- Be sure to make and go to all appointments
- Take your medicines exactly as prescribed for as long as they are prescribed.
- While recovering from your surgery, practice leg lifts while your feet are elevated and try to break up your day to ambulate with crutches so you can walk on your good side.
- Follow up with your surgery team as to when you can begin physical therapy